Psoriasis vs Eczema: Key Differences, Symptoms & Treatment
Psoriasis vs Eczema: What’s the Real Difference?
You notice a red, itchy patch of skin and start searching for answers. The photos online show two conditions that look frustratingly similar — red, inflamed, scaly. You’re trying to tell the difference between psoriasis and eczema, and you’re not alone in finding it genuinely confusing.
Even dermatologists occasionally need a skin biopsy to distinguish them with certainty. That’s not a failure of observation — it’s a reflection of how much overlap exists in how psoriasis vs eczema can appear, especially in early or atypical presentations. But the two conditions have completely different underlying causes, predictably different locations on the body, and require meaningfully different treatment approaches.
This guide gives you the clinical detail, the visual language, and the practical knowledge to understand what separates them — and when to see a doctor.
What Is Psoriasis? A Clinical Overview
Psoriasis is a chronic autoimmune disease in which an overactive immune system — driven by T-cells — dramatically accelerates the skin cell lifecycle, causing cells to build up on the surface and form thick, red plaques covered with silvery-white, flaking scales.
In healthy skin, cells move from the inner layers to the surface over about 28 to 30 days before shedding. In psoriasis, that cycle can compress to just 3 to 5 days. Cells don’t have time to shed naturally; they pile up, producing the characteristic plaques.
According to the National Psoriasis Foundation, psoriasis affects approximately 7.5 million adults in the United States and between 2 and 3 percent of the global population. It is not a skin disease in isolation — it’s a systemic immune condition. Roughly 30 percent of people with psoriasis develop psoriatic arthritis, which causes joint pain, swelling, and can lead to permanent joint damage if untreated.
Plaque psoriasis (psoriasis vulgaris) is the most common form, accounting for approximately 80 to 90 percent of cases. Other forms include guttate (small teardrop-shaped spots, often triggered by streptococcal infection), inverse (smooth lesions in skin folds), pustular (pus-filled blisters), and erythrodermic (severe, widespread reddening affecting most of the body — a medical emergency).
Genetic factors play a significant role. Having a first-degree relative with psoriasis raises a person’s risk considerably, and specific genes — particularly those within the HLA-C locus — are strongly associated with disease susceptibility. However, genetics alone don’t determine who develops it; environmental triggers play an equally important role.
Common psoriasis triggers include:
- Psychological stress (one of the most consistently reported)
- Streptococcal throat infection (especially in guttate psoriasis)
- Skin injury or trauma — the Koebner phenomenon, where psoriasis develops at sites of cuts, burns, or tattoos
- Heavy alcohol consumption and smoking
- Certain medications: beta-blockers, lithium, antimalarials, and NSAIDs in some individuals
- Hormonal changes
What Is Eczema (Atopic Dermatitis)? A Clinical Overview
Eczema, most commonly referring to atopic dermatitis, is a chronic inflammatory skin condition characterized by a dysfunctional skin barrier that fails to retain moisture and protect against environmental irritants and allergens, resulting in dry, intensely itchy, red, and inflamed skin.
The word “atopic” places eczema within the atopic triad — the tendency to develop atopic dermatitis, asthma, and allergic rhinitis (hay fever). These three conditions frequently coexist in the same individual, and the progression from eczema in infancy to asthma and allergies in childhood is so commonly observed that it has a clinical name: the atopic march.
The National Eczema Association estimates that over 31 million Americans live with some form of eczema. Globally, atopic dermatitis affects up to 20 percent of children and between 1 and 3 percent of adults, according to data published in the Journal of Allergy and Clinical Immunology. It often begins in infancy or early childhood — many children experience significant improvement by adolescence, though for a substantial number it persists into adulthood or re-emerges later in life.
At the cellular level, eczema involves both a defective skin barrier (frequently linked to mutations in the gene encoding filaggrin, a structural protein essential to healthy skin) and immune dysregulation, particularly an overactive Th2 immune response that promotes inflammation and hypersensitivity to environmental triggers.
Common eczema triggers include:
- Harsh soaps, detergents, and cleaning products
- Fragrances and preservatives in skincare products
- Dry, cold air or low-humidity environments
- Dust mites, pet dander, and mold
- Certain foods — dairy, eggs, peanuts, tree nuts, soy, and wheat in some individuals, particularly children
- Sweat and heat
- Psychological stress
- Wool and synthetic fabrics in direct contact with skin
Psoriasis vs Eczema: 7 Key Differences
This is the most practical section for distinguishing the two conditions. The differences are real and clinically meaningful — understanding them helps you communicate more clearly with your doctor and supports faster, more accurate diagnosis.
Master Comparison Table
| Feature | Psoriasis | Eczema (Atopic Dermatitis) |
|---|---|---|
| Root Cause | Autoimmune (T-cell driven overproduction of skin cells) | Skin barrier dysfunction + Th2 immune dysregulation |
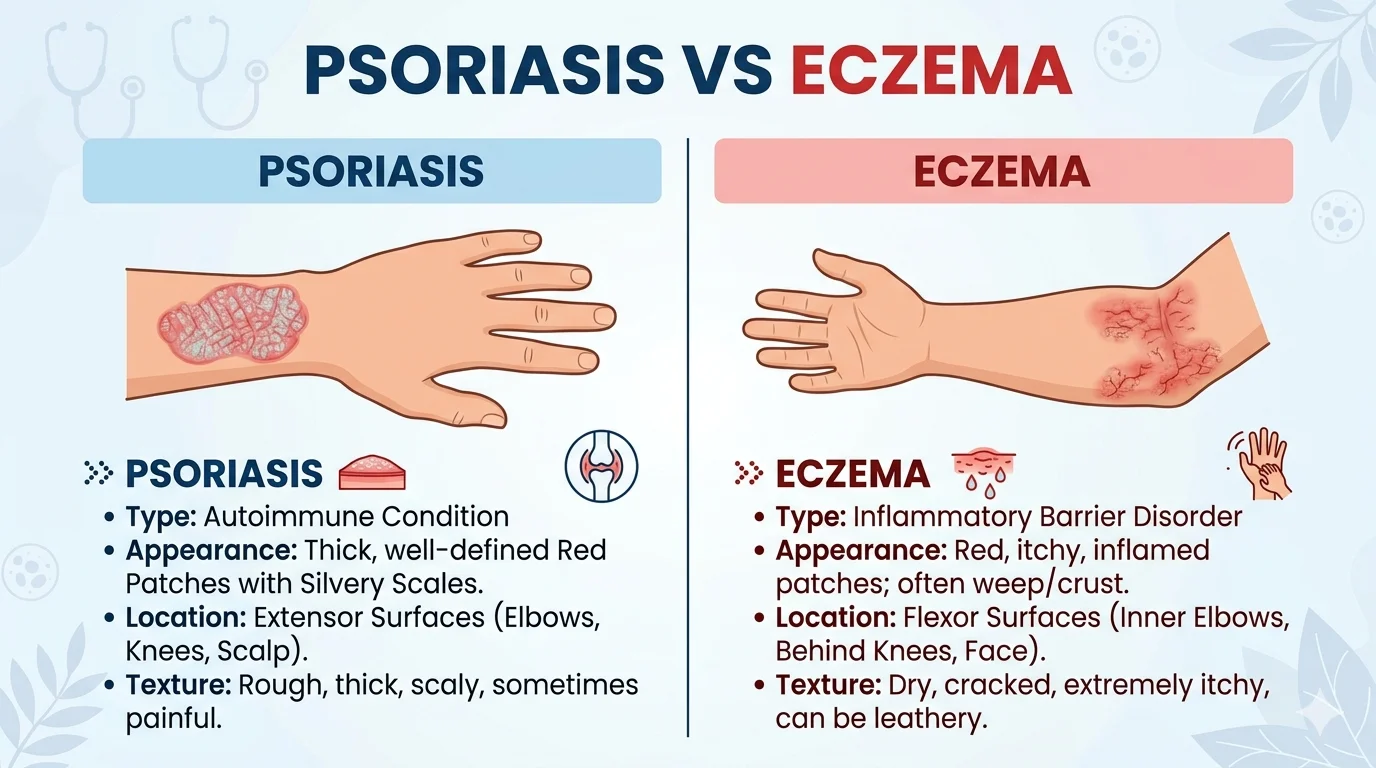
| Appearance | Thick, salmon-pink or red plaques with micaceous silvery-white scale | Dry, red, scaly patches; may weep fluid, crust, or become lichenified (thickened) |
| Borders | Well-defined, sharply demarcated edges | Ill-defined, diffuse, blending into surrounding skin |
| Itch Level | Variable — mild to moderate in many cases, though can be severe | Typically intense and relentless, often dramatically worse at night |
| Primary Locations | Scalp, extensor elbows and knees, lower back, nails, genitals | Flexural areas: inner elbows, behind knees; also face, hands, neck, wrists |
| Age of Onset | Bimodal: peaks at 20–30 and 50–60 years; can occur at any age | Most commonly begins before age 5; often improves with age |
| Koebner Phenomenon | Present — rash develops at sites of skin trauma or injury | Not a feature of eczema |
| Nail Involvement | Frequent — pitting, onycholysis, “oil drop” discoloration | Less common |
| Associated Conditions | Psoriatic arthritis (~30%), cardiovascular disease, metabolic syndrome | Asthma, allergic rhinitis, food allergies (atopic triad) |
| Skin Biopsy Finding | Munro’s microabscesses (neutrophils in stratum corneum) | Spongiosis (intercellular edema in epidermis) |
Breaking Down the Differences
1. The Root Cause is Fundamentally Different
Psoriasis is driven by an immune system error — T-cells mistakenly attack healthy skin cells, triggering an inflammatory cascade that accelerates skin cell turnover dramatically. It is classified as an autoimmune disease, and this classification shapes everything about treatment.
Eczema’s origin is a two-part failure: a genetically compromised skin barrier that allows irritants, allergens, and microbes to penetrate too easily, combined with a hypersensitive immune response that reacts with disproportionate inflammation. It is not autoimmune in the strict sense; it is inflammatory, allergic, and barrier-mediated.
2. The Visual Presentation Tells a Story
Psoriasis plaques are distinctive: well-defined, almost geometric in their edges, with a characteristic thick, silver-white scale that — when scraped — can flake off in layers (this is called the Auspitz sign, where removing the scale reveals pinpoint bleeding beneath). On darker skin tones, the appearance may be more violet or brown than pink, with less obvious silvery scaling.
Eczema rashes are messier in their geography. The edges blur into surrounding skin. In acute flares, affected areas may weep clear or yellowish fluid and develop honey-colored crusting — a sign that secondary bacterial infection (commonly Staphylococcus aureus) has developed, which is a frequent complication. In chronic eczema, repeated scratching produces lichenification: the skin thickens, hardens, and develops exaggerated skin markings, giving it a leathery texture.
3. Location Is a Powerful Diagnostic Clue
Psoriasis has a strong preference for extensor surfaces — the outer elbow, the knee, the scalp, and the lower back. These are areas exposed to friction and pressure, which relates to the Koebner phenomenon. Nail psoriasis — pitting, separation from the nail bed, or “oil drop” amber discoloration under the nail — occurs in up to 50 percent of psoriasis patients and is a significant clue.
Eczema gravitates toward flexural surfaces — the inner elbow crease, the skin behind the knees, the neck, the eyelids, and in infants, the face and scalp. In adults, hands are a very common site. The pattern makes biomechanical sense: skin folds trap sweat and irritants, and in compromised barrier skin, these exposures trigger and maintain inflammation.
4. The Nature of the Itch Differs
Eczema itch is categorized differently from psoriasis itch in clinical literature. The itch of eczema is often described by patients as “unbearable,” “maddening,” or “impossible to ignore.” It is prominently nocturnal, disrupting sleep night after night. The resulting itch-scratch cycle — where scratching further damages the barrier, which worsens inflammation, which intensifies itch — is one of the most challenging aspects of managing atopic dermatitis. Children scratch until they bleed in their sleep.
Psoriasis itch, while present and sometimes severe, is more variable. Many patients describe it as a burning or stinging sensation more than a pure urge to scratch. The pain of cracked, bleeding plaques on the hands or scalp is often what troubles psoriasis patients more than itch alone.
5. Psoriasis Can Injure Its Own Skin (Koebner Phenomenon)
One of the more striking features of psoriasis is the Koebner phenomenon: new psoriatic plaques can develop within weeks at sites of skin injury — a cut, a sunburn, a surgical scar, a tattoo. This does not occur in eczema. Its presence is a useful clinical clue when the diagnosis is in question.
Visual Clues: Recognizing Each Condition on the Body
What psoriasis looks like: On the elbow, imagine a patch of skin that looks almost laminated — thick, with white or silvery “paint-like” scale that seems applied on top rather than part of the skin itself. The edges are crisp, almost like the border was drawn. On the scalp, plaques may extend slightly beyond the hairline. Fingernails may show tiny ice-pick pits or separate from the nail bed at the free edge.
What eczema looks like: On the inner elbow, picture raw, angry, reactive skin — reddened and swollen in flares, then leathery and hyperpigmented when chronic. It doesn’t have the defined edge of psoriasis. In severe cases, small blisters (vesicles) may form. Around the eyes, eczema can cause darkening of the lower lids (sometimes called “allergic shiners”) and fine horizontal creases (Dennie-Morgan lines), both classic signs in atopic individuals.
On darker skin tones, both conditions often present with greater hyperpigmentation and less redness, making them harder to identify through photographs calibrated to lighter skin. Psoriasis may appear more violaceous (purple-tinged) than red. Eczema post-inflammatory hyperpigmentation can persist long after the active inflammation resolves. A dermatologist experienced with diverse skin tones is valuable — clinical photography references for darker skin remain underrepresented in standard dermatology resources.
Itch, Pain, and Quality of Life: Living With These Conditions
The numbers in clinical studies rarely capture what daily life looks like for people managing either condition.
For eczema patients, sleep deprivation is one of the most-documented consequences. Research published in the British Journal of Dermatology has documented significant impairment in sleep quality in both adults and children with moderate-to-severe atopic dermatitis, with downstream effects on mood, cognitive performance, and school or work productivity. The visible nature of eczema — redness, swelling, crusting on hands or face — carries a significant psychosocial burden. Anxiety and depression rates are measurably elevated in the eczema population compared to the general public.
For psoriasis patients, the plaques themselves can be physically painful — especially when they crack and bleed. Psoriasis on the palms or soles of the feet makes everyday activities — gripping objects, walking — actively painful. The 30 percent of psoriasis patients who develop psoriatic arthritis face an additional layer: joint inflammation, stiffness, and in severe untreated cases, progressive joint destruction. The emotional weight of a visible, chronic, misunderstood skin disease compounds the physical symptoms significantly.
Both conditions are associated with higher rates of depression, anxiety, and social withdrawal. Neither is trivial in its impact on life quality.
Triggers and Causes: Why These Conditions Develop
Understanding what provokes flares is essential to managing either condition — and the trigger lists, while overlapping in some places (stress is common to both), are meaningfully different.
Psoriasis is primarily driven internally. The immune system is dysregulated at a genetic and cellular level, and external triggers provoke flares by activating that already-primed response. This is why systemic treatments that modulate the immune system — biologics, methotrexate, cyclosporine — are so central to psoriasis management.
Eczema is primarily driven externally meeting an internal vulnerability. The skin barrier cannot defend itself against irritants and allergens that healthy skin manages without difficulty. Identifying and eliminating individual triggers is central to eczema management in a way that isn’t equally true for psoriasis.
Stress operates differently in the two conditions: in psoriasis, stress triggers immune activation that drives plaques; in eczema, stress can both worsen the itch-scratch cycle directly (stress hormones lower the itch threshold) and impair barrier recovery.
Diagnosis: How Dermatologists Tell Them Apart
Clinical diagnosis relies first on visual examination by an experienced dermatologist. Location, morphology, border characteristics, nail involvement, and family history together form a clinical picture that guides diagnosis in the majority of cases.
Dermatoscopy (dermoscopy) — examining the skin under a handheld magnifying instrument — adds detail: the regular dotted or glomerular vascular pattern of psoriasis differs from the non-specific pattern typical of eczema.
When the clinical picture is ambiguous, a punch biopsy provides histological certainty. The pathology differs clearly:
- Psoriasis shows Munro’s microabscesses — small collections of neutrophils within the stratum corneum — along with regular epidermal thickening (acanthosis) and elongated rete ridges.
- Eczema shows spongiosis — intercellular fluid accumulation in the epidermis — with a predominantly T-lymphocyte infiltrate. There are no neutrophil microabscesses.
Patch testing may also be ordered if contact allergens are suspected in eczema.
Treatment: What Works for Each Condition
Treatment strategies differ substantially because the underlying mechanisms differ. What follows reflects current clinical practice as of 2026; treatment in both fields is advancing rapidly.
Treatment Comparison Table
| Treatment Type | Psoriasis | Eczema (Atopic Dermatitis) |
|---|---|---|
| Topical Corticosteroids | First-line for mild-to-moderate; various potencies by location | First-line; used cautiously on face, eyelids, and skin folds due to atrophy risk |
| Vitamin D Analogs | Calcipotriene (Dovonex), calcitriol — effective, especially in combination with steroids | Not used |
| Topical Calcineurin Inhibitors | Off-label for sensitive areas (face, genitals) | Approved: tacrolimus (Protopic), pimecrolimus (Elidel); steroid-sparing agents |
| Topical JAK Inhibitors | Emerging use | Ruxolitinib cream (Opzelura) — FDA-approved for mild-to-moderate atopic dermatitis |
| Coal Tar / Anthralin | Used, particularly for scalp psoriasis | Occasionally for chronic lichenified eczema |
| Phototherapy | Narrowband UVB and PUVA — highly effective | Narrowband UVB used in moderate-to-severe cases |
| Systemic Oral Medications | Methotrexate, cyclosporine, acitretin, apremilast (Otezla) | Cyclosporine, methotrexate (for severe, refractory cases) |
| Biologics | Anti-TNF: adalimumab (Humira), etanercept; IL-17: secukinumab (Cosentyx), ixekizumab; IL-23: risankizumab (Skyrizi), guselkumab | Dupilumab (Dupixent) — anti-IL-4/IL-13; tralokinumab (Adbry) |
| Oral JAK Inhibitors | Deucravacitinib (Sotyktu) — TYK2 inhibitor approved for plaque psoriasis | Upadacitinib (Rinvoq), abrocitinib (Cibinqo) — for moderate-to-severe AD |
| Emollients / Moisturizers | Helpful adjunct | Central to management; applied immediately after bathing |
A critical distinction: Dupilumab (Dupixent) — currently the most prescribed biologic for moderate-to-severe atopic dermatitis — targets the IL-4 and IL-13 signaling pathways that drive atopic inflammation. It is not effective for psoriasis. Conversely, IL-17 inhibitors like secukinumab, among the most effective psoriasis biologics, have no role in eczema management and could theoretically worsen atopic disease by shifting the immune balance. Treating the wrong condition with a condition-specific biologic is clinically meaningless at best and potentially harmful — which is why accurate diagnosis before systemic treatment is non-negotiable.
Living With Psoriasis or Eczema: Practical Daily Management
Beyond prescription treatments, daily habits significantly affect disease burden for both conditions.
For psoriasis:
- Moisturize consistently — while not as central as in eczema, keeping plaques hydrated reduces scale and discomfort. Look for thick creams or ointments rather than lightweight lotions.
- Avoid skin trauma where possible — remember the Koebner phenomenon. Minor cuts and abrasions can seed new plaques.
- Consider dietary influences. While no single diet treats psoriasis, an anti-inflammatory eating pattern — more omega-3 fatty acids, less processed food and alcohol — correlates with lower inflammatory burden in some observational studies.
- Smoking cessation matters. Smoking is associated with worse psoriasis severity and poorer treatment response.
- Seek support. The National Psoriasis Foundation’s online community connects patients with peer support and treatment resources.
For eczema:
- The wet wrap technique during flares — applying moisturizer under a damp then dry bandage layer — can provide significant short-term relief and help topical treatments penetrate more effectively.
- Bathe in lukewarm (not hot) water for 10–15 minutes, then apply emollient within 3 minutes of patting dry — while skin is still slightly damp. This is the “soak and seal” method recommended by the National Eczema Association.
- Identify and eliminate personal triggers systematically. A symptom and trigger diary, maintained over several weeks and reviewed with a dermatologist or allergist, is more reliable than general elimination guessing.
- Dust mite reduction measures — mattress covers, frequent washing of bedding at 60°C or higher, HEPA filtration — help a meaningful proportion of eczema patients for whom dust mite allergy is a documented trigger.
- Fragrance-free, dye-free laundry detergents and personal care products reduce baseline irritant load.
When to See a Doctor
See a dermatologist if:
- A rash does not improve with basic moisturizing after 2 weeks
- Itching disrupts sleep regularly
- Skin is cracking, bleeding, or showing signs of infection (increasing redness, warmth, pus, or spreading)
- Joints are painful, swollen, or stiff alongside skin symptoms (psoriatic arthritis can develop before or after skin symptoms)
- Over-the-counter treatments are providing insufficient relief
Do not attempt to self-diagnose or self-treat moderate-to-severe disease based on internet descriptions alone. Biopsy-level accuracy sometimes requires a specialist.
Glossary of Key Dermatological Terms
| Term | Definition |
|---|---|
| Atopic triad | The tendency for atopic dermatitis, asthma, and allergic rhinitis to coexist in the same individual |
| Koebner phenomenon | Development of psoriatic plaques at sites of skin trauma |
| Lichenification | Thickening and hardening of skin from chronic rubbing or scratching |
| Spongiosis | Intercellular fluid in the epidermis; hallmark of eczema on biopsy |
| Munro’s microabscesses | Neutrophil clusters in the skin’s outer layer; hallmark of psoriasis on biopsy |
| Auspitz sign | Pinpoint bleeding revealed when psoriatic scale is removed |
| Atopic march | Progression from eczema in infancy to asthma and allergic rhinitis in childhood |
| Filaggrin | Structural skin protein; mutations impair skin barrier function in eczema |
| Biologic | A targeted therapy derived from biological sources; inhibits specific immune pathways |
| JAK inhibitor | Small molecule drugs that block Janus kinase signaling involved in immune-driven inflammation |
FAQ SECTION
Can you have both psoriasis and eczema at the same time? Yes, though it is uncommon. Having both simultaneously is called “psoriasis-eczema overlap” and presents a diagnostic challenge. In such cases, biopsy findings and clinical history help separate the conditions. Treatment must address both, and some systemic agents used for one may conflict with management of the other.
Is psoriasis or eczema more common? Eczema (atopic dermatitis) is significantly more common globally — affecting up to 20 percent of children and 1–3 percent of adults. Psoriasis affects approximately 2–3 percent of the global population. In absolute numbers, atopic dermatitis is one of the most prevalent chronic skin conditions in the world, particularly in childhood.
Does psoriasis itch like eczema? Both conditions can cause itching, but the itch is different in character. Eczema itch is typically intense, relentless, and worst at night, often creating a destructive itch-scratch cycle. Psoriasis itch is more variable — present in many patients, sometimes severe, but more often described as burning or stinging, and less consistently nocturnal.
Can psoriasis turn into eczema or vice versa? No. These are biologically distinct conditions with different genetic bases, cellular mechanisms, and immune pathways. One does not transform into the other. However, a person can receive an incorrect diagnosis initially — misidentifying eczema as psoriasis or vice versa — and then receive a corrected diagnosis as the condition evolves or is biopsied.
Is psoriasis contagious like eczema? Neither psoriasis nor eczema is contagious in any way. Psoriasis is an autoimmune condition; eczema is a skin barrier disorder with immune involvement. Neither can be transmitted through skin-to-skin contact, sharing objects, or any other route. Both arise from internal genetic and immune factors.
How can I determine whether I have psoriasis or eczema? The strongest self-identification clues are location and appearance: if thick, silvery-scaled patches appear on the outer elbows, knees, or scalp with crisp edges, psoriasis is more likely. If an intensely itchy rash appears in skin creases — inner elbows, behind knees — with blurred borders and possibly weeping or crusting, eczema is more likely. A dermatologist’s examination, and sometimes a biopsy, is needed for certainty.
Conclusion
Psoriasis and eczema are two distinct diseases that happen to share a surface address — the skin — and occasionally similar visual appearances. The difference between psoriasis and eczema, once you understand the underlying biology, is fundamental: one is an immune system attacking the skin’s own production cycle; the other is a skin that cannot protect itself triggering disproportionate immune responses.
Clinically, the location, border sharpness, scale type, associated symptoms, age of onset, and biopsy findings draw a clear line between them in most cases. The treatments work along completely different pathways.
If you’re living with either condition and finding current management insufficient, the landscape of available treatments has changed substantially over the past decade. New biologics and JAK inhibitors have transformed moderate-to-severe disease in both categories. A conversation with a board-certified dermatologist about current options is worth having.
Next: Explore our detailed guide on Atopic Dermatitis Explained for a deeper look at eczema’s types, triggers, and emerging treatments.